中心的なコンセプト
この記事では、最も一般的に使用されているいくつかの新型コロナウイルス感染症治療薬の基礎となる生化学的基礎を調査します。それらの作用機序、薬物動態原理、恐るべき SARS-CoV-2 ウイルスとの闘いにおける有用性について学びます。また、医薬品の標的、抗ウイルス耐性の問題の増大、および補足的および補完的な 新型コロナウイルス感染症 (COVID-19) 治療の選択肢についても理解します。
これはケーススタディとして新型コロナウイルス感染症 (COVID-19) を使用し、化学と公衆衛生の交差点に関する特別な ChemTalk ミニシリーズの 5 番目の記事です。このシリーズ全体を通じて、創薬と開発のプロセス、病気の診断と予防における化学の中心的な役割、化学と公衆衛生の最前線で働くキャリアについて学ぶことが期待できます。
このミニシリーズの他の記事
コロナウイルスの背後にある化学
創薬プロセス
医薬品開発プロセス
公衆衛生分野における化学のキャリア
検査室診断による病気発見の仕事
疾病予防のための科学的戦略
化学、公衆衛生、そしてあなた
新型コロナウイルス感染症 (COVID-19) は医薬品開発プロセスにどのような影響を与えましたか?
ここまでで、私たちは製薬プロセスの厳重な手順と、医薬品を作成する多くの生物医学の専門家を見学してきました。これは、医薬品開発がどのようなものであるかについての「通常の」状況を表しています。しかし、パンデミックのような健康危機の際には、疫学的な状況が急速に変化するため、その状況も急速に変化する可能性があります。
新型コロナウイルス感染症(COVID-19)に対する公衆衛生上の対応は、多くの変動部分を両立させた。特定の都市が局地的流行を抑えるたびに、別の場所でまるで間断なく新たな流行が発生した。業界全体が深刻な経済的影響を受けましたが、一部の業界は現在も回復を続けています。長期にわたる社会的孤立の影響で、私たちの相互交流の方法が変化し、一部の人々の精神的健康に影響を与えました。その間ずっと、医療従事者は医療インフラが逼迫している中で、押し寄せる患者を管理しなければなりませんでした。
パンデミックの開始時に変更する必要があったもう 1 つの要素は、医薬品開発プロセスでした。通常、非常に組織化され、標準化された作戦が、パンデミックの進化する社会、経済、政治的状況に対応するために突然急遽変更されました。生物医学研究者は、新型コロナウイルス感染症 (COVID-19) の治療薬の作成とテストに協力して取り組み、最終的には、新型コロナウイルス (COVID-19) の原因である SARS-CoV-2 を正確に特定する新しい薬とワクチンを製造することに成功しました。
この記事では、いくつかの代表的な新型コロナウイルス感染症治療薬がどのように作用し、それらが包括的なパンデミック対応にどのように適合するかに焦点を当てます。ここでは、この大局的な視点から一歩下がって、これらの医薬品がどのようにして現代における最悪の健康危機の 1 つを回避するのに役立ったかについて、より小規模な詳細に焦点を当ててみましょう。
抗ウイルス薬が新型コロナウイルス感染症の治療法として使用されるのはなぜですか?
新型コロナウイルス感染症の治療薬は SARS-CoV-2 ウイルスを標的としているため、 一種の抗ウイルス薬となります。 。他の病原体と比較して、ウイルスは特に治療が難しい場合があります。その理由については、後ほど詳しく説明します。最も厳密な意味でウイルス性疾患を「治療」したり根絶したりすることはできませんが、ウイルスが消滅するまでの間、症状を管理することはできます。抗ウイルス薬は多くの場合、身体症状を緩和し、患者が回復するまでに他の人への病気の蔓延を防ぐことを目的としています。
抗ウイルス薬は抗生物質薬とは全く対照的です。 、病原体が細菌である感染症の治療に使用されます。抗生物質にはその役割がありますが、新型コロナウイルス感染症は細菌ではなくウイルスによって引き起こされるため、抗生物質は決して現実的な新型コロナウイルス感染症の治療選択肢ではありませんでした。抗生物質が使用する細菌を殺す技術は、ウイルスを倒すことには何の役にも立ちません。それはフォークでスープを食べようとするようなものです。
その代わりに、ウイルスに勝つのにふさわしい薬を作り出さなければなりません。抗ウイルス薬を開発するとき、研究者はまず、その特定のウイルスがどのように作用するか、つまり、ウイルスがどのように体内に侵入するか、どのように健康な細胞に感染するか、どのように人の間で広がるかなどを評価します。ウイルスのメカニズムを理解することで、研究者は薬のメカニズムを決定することができます。薬はウイルスの通常の機能を中断または最小限に抑えるように作用する必要があります。
この戦略的アプローチは、 より広範な創薬の初期段階を反映しています。 このプロセスを通じて、生物医学科学者は医薬品を設計する最初のステップを踏みます。 SARS-CoV-2 のようなコロナウイルスは、健康な細胞の分子生物学機構を乗っ取って、自身の遺伝物質を複製します。これを知った研究者たちは、ウイルスが宿主細胞に侵入したり利用したりする能力を妨げる薬剤の設計に注力しました。これらのプロセスを抑制できれば、SARS-CoV-2 とパンデミック全体も抑制できる可能性があります。そこで、次の重要な疑問が生じました。SARS-CoV-2 の典型的な戦術を妨げる抗ウイルス薬をどのようにして作ることができるでしょうか?
この記事のミニシリーズの前半で、日常的な創薬技術と 2 つの例の薬剤がどのように機能するかについて説明したことを覚えているかもしれません。このセクションでは、これらの新型コロナウイルス感染症治療薬の 1 つとその前例の開発について、化学の観点から再検討します。この課題は、パンデミックを解決するための科学者のアプローチの指針となりました。生物医学研究者が指揮する製薬研究所はすぐにミッションコントロールセンターになりました。しかし、新型コロナウイルス感染症の治療薬を開発するために、これらの研究所内で一体何が起こったのでしょうか?
新型コロナウイルス感染症の治療薬をマスターする
2020 年初頭、SARS-CoV-2 が世界中で活発に大混乱を引き起こす中、新型コロナウイルス感染症 (COVID-19) の治療薬の探索が進められています。世界中の研究チームが独立して協力して、この猛獣を打ち負かす薬剤候補を開発しています。しかし、そのプロセスには何が必要なのでしょうか?そして、それは痛みの軽減を待ち望んでいる患者にとって何を意味するのでしょうか?
新型コロナウイルス感染症(COVID-19)がパンデミックにまでエスカレートすると、科学者たちは無駄な時間はないことを悟りました。患者、医療従事者、企業、政府、一般大衆は、簡単に配布できる安全で効果的な治療法の開発を彼らに期待していました。病気の急速な蔓延とその背景で起きているサプライチェーンの課題を考慮すると、これらの医薬品の特性は極めて重要でした。現在最も一般的な新型コロナウイルス感染症治療薬 (これらの基準を達成したもの) の 1 つは、ニルマトレルビル/ リトナビル と呼ばれる抗ウイルス薬です。 。この薬については、Paxlovid というブランド名でよく知られているかもしれません。生物医学科学者たちが、たとえ時間ギリギリであったとしても、どのようにしてこのような新型コロナウイルス感染症治療薬を開発したかについて簡単に説明しましょう。
誰もが大好きなカムバックストーリー:新型コロナウイルス感染症治療薬の開発
理想的な新型コロナウイルス感染症治療薬の特性を特定したばかりの製薬研究者の(黙った)立場になって考えてみましょう。次に、最も重要な部分、そしておそらくあなたが直面する最大の障害が来ます。それは、実際にどうやって成功するのかということです。いくつかの前駆体物質の化学を操作して、目的の分子を生成するにはどうすればよいでしょうか?薬を効果的にするための品質がすでに決定されているので、今度は薬自体を作るプロセスを慎重に検討する必要があります。これを、新型コロナウイルス感染症の治療薬として使用される 3 つの化合物に照らして評価します。
ニルマトレルビル/リトナビルおよびルフォトレルビル
強力な合成ルートから必要なものがいくつかあります。最良の合成アプローチは、医薬品開発の経済的コストを最小限に抑えるために、出発物質をほとんど使用しないことです。また、迅速な反応を採用し、医薬品の製造プロセスを加速して、医薬品をより早く患者に届けることができます。 (この点は、パンデミックの最も激しい波の最中に新型コロナウイルス感染症の治療薬を製造する際に特に価値がありました!) また、薬剤の純度を最大化し、不必要な無駄を避けるために、副産物をできるだけ少なくする戦略も望んでいます。少ない労力で高収率の化学合成は、製薬メーカーの収益を向上させ、最終的にはより効率的な医薬品生産につながります。
研究者らはリトナビル(すでにHIV薬として存在していた)を新型コロナウイルス感染症(COVID-19)の治療に再利用したが、ニルマトレルビルはゼロから合成された。これは別の分子であるルフォトトレビルの子孫です。 、実際に新型コロナウイルス感染症の臨床試験でも研究されています。すぐに説明するように、ニルマトレルビルとルフォトレルビルの違いは、作用の仕方 (どちらもプロテアーゼ阻害剤) ではなく、患者の体に送達される方法にあります。
パンデミックを克服するには?キャー、問題ありません!
医薬品開発では、同じ最終製品を達成するために複数の手段が存在することがよくあります。最も重要なことは、最終的に得られる分子が適切な位置に適切な官能基を持っているかどうか、そして治療目的を達成できるかどうかです。目的の化合物の分子骨格が出発物質にすでに存在しているため、既存の化合物から新しい化合物を合成することは簡単な選択肢になる傾向があります。ニルマトレルビルを作るために、科学者たちはトリペプチド鎖の骨格から始めました。
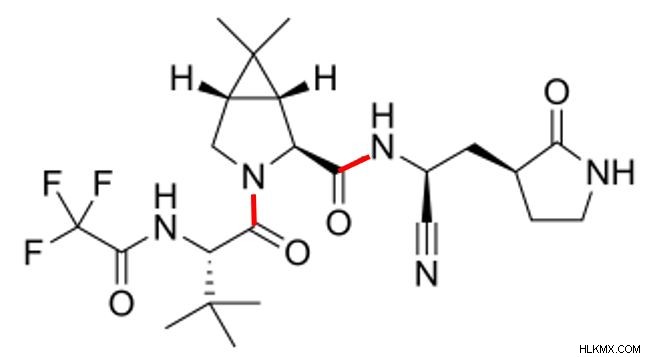 ニルマトレルビルの化学構造。 2 つのペプチド結合とシアノ官能基に特に注意してください。
ニルマトレルビルの化学構造。 2 つのペプチド結合とシアノ官能基に特に注意してください。 この分子形態について理解すべき重要な点が 2 つあります。まず、ニルマトレルビルをよく見ると、その構造内に 2 つのペプチド結合が見られます (上で赤で強調表示されています)。これは、ニルマトレルビルが 3 つのペプチドが結合して構成されているという手がかりです。この場合、問題の 3 つのペプチドは自然界には存在しません。合成化学者がそれらを改変したのです。ニルマトレルビルの合成には、一連の縮合反応を実行してペプチド結合を形成し、単一分子内で 3 つのペプチドを結合することが含まれます。
ニルマトレルビルを構成するペプチドは自然界には存在しないため、 ニルマトレルビルはペプチド模倣薬です。 分子。ペプチド模倣物はペプチドに似ており、その機能を模倣しますが、合成であるため、天然のタンパク質が示す問題を回避できることがよくあります。対象となるペプチド模倣分子によっては、実際のペプチドよりも優れた安定性、選択性、または効力を示す場合があります。これらすべての要因が、体内での持続時間や目的の病原体をどれだけうまく標的にするかなど、薬の効果に影響を与えます。したがって、ペプチド模倣薬の最大の利点は、研究者が化学合成を通じて特定の治療計画のニーズに合わせてその挙動をカスタマイズできることです。常に移動し、特定することが難しいウイルスと戦う場合、オーダーメイドのペプチド模倣薬は熱追尾ミサイルのようなもので、非常に正確で標的をしっかりと捉えます。
第二に、ニルマトレルビルは炭素-窒素三重結合の誇り高き所有者であり、その祖先であるルフォトレルビルには存在しない特徴であることがわかります。高エネルギーで比較的不安定なシアノ基 ニルマトレルビルの新型コロナウイルス感染症治療薬としての機能にとって重要です。 「求電子弾頭」 と呼ばれるそれは主要なプロテアーゼを標的とする存在です。 (プロ )SARS-CoV-2の複製を促進します。ニルマトレルビルのシアノ基が Mpro のシステイン残基と直接接触すると、ウイルスが複製に使用するタンパク質を生成する Mpro の能力が阻害されます。コロナウイルスファミリーのメンバーの中で、Mpro 分子は高度に保存されています。それは、ニルマトレルビルがウイルスのライフサイクルにおいて基本的な役割を担っているためですが、この保存により、ニルマトレルビルはいくつかの異なるコロナウイルス変異種と戦うことができるようになります。このような小さな原子のペアが、薬の機能、そしてもちろん患者の予後に重大な影響を与えるということは、非常に深いことです。
バディ システム:新型コロナウイルス感染症との戦いにおけるリトナビルの役割
ただし、ニルマトレルビルだけではこれらすべてを行うことはできません。別の化合物であるリトナビルのサポートを利用すると、この困難な取り組みを一緒に実行できるため、より効果的に機能します。患者がニルマトレルビルを服用すると、(他の錠剤と同様に)体内の消化器系の代謝の猛威にさらされます。 (これについては後ほど詳しく説明します。) 現時点では、時間の経過とともに体の消化力によって錠剤が分解されることを理解してください。錠剤の分解が早いほど、治療効果の持続期間は短くなります。
したがって、ニルマトレルビルのような新型コロナウイルス感染症治療薬の効果をより長期間持続させるには、体内の治療薬の代謝を遅らせる方法を見つける必要があります。ここがリトナビルが輝くところです。リトナビルの唯一の仕事は、ニルマトレルビルの分解を減らし、ニルマトレルビルがより長く作用できるようにすることです。リトナビルはCYP3A4を阻害します。 、肝臓に豊富に見られるシトクロムであり、薬物代謝を触媒します。分解が阻害されたことで、ニルマトレルビルは通常なら代謝する酵素をうまく回避できるようになりました。これにより、患者はリトナビルが存在しなかった場合よりもニルマトレルビルの治療効果をより長く経験することができます。
 リトナビル分子。この画像の上部近くにある 2 つのチアゾール環に注目してください。
リトナビル分子。この画像の上部近くにある 2 つのチアゾール環に注目してください。 CYP3A4 の阻害を可能にするリトナビルの構造の何が特別なのでしょうか? 2つのチアゾール基です! チアゾール 基は、5 つの原子 (窒素と硫黄を含む) と 2 つの二重結合を持つ複素環です。リトナビルでは、これらのチアゾール基が 2 つの非常に重要な方法で薬剤の効果をサポートすることで二重の役割を果たします。構造的な観点から見ると、各リングはリトナビルの他のほとんどの成分よりもはるかに大きいです。分子の両端にチアゾール基を配置すると、リトナビルの全体的な安定性が高まり、構造がより堅牢になります。
チアゾール基のもう 1 つの重要な目的は、リトナビルが CYP3A4 と相互作用する場所であることです。 CYP3A4 にはヘムが含まれています。 鉄原子を含む基。リトナビルのチアゾール基の窒素はこの鉄原子と密接に結合し、高い結合親和性でこの選択的相互作用を推進します。実際、この結合は非常に強力であるため、元に戻すことはできません。そうは言っても、体は最終的にリトナビルとニルマトレルビル分子を必然的に代謝します。いずれにせよ、この超特異的かつ不可逆的な結合作用により、薬の効果がそうなる前にできるだけ長く持続することが保証されます。
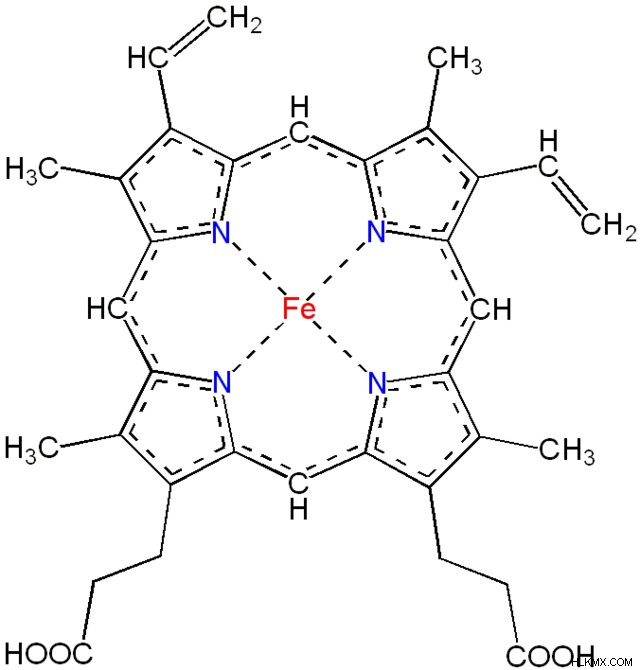 ヘム グループの構造の概要。鉄原子 (赤色) と非局在化電子 (破線) を示します。リトナビルのチアゾール基は鉄と結合して、CYP3A4 の代謝活性を阻害します。
ヘム グループの構造の概要。鉄原子 (赤色) と非局在化電子 (破線) を示します。リトナビルのチアゾール基は鉄と結合して、CYP3A4 の代謝活性を阻害します。 変化を受け入れる:プロドラッグがどのように活性型に変化するか
さて、ニルマトレルビルの前身であるルフォトレルビルをもう一度見てみましょう。ルフォトトレビルが血流に到達すると、 酵素アルカリホスファターゼが働きます。 かなり急速に活性型に切断されます。そのため、 ルフォトレビル自体はプロドラッグです。 、 薬物の活性型の不活性前駆体であり、生体内で活性型に変換されます。 。薬物の活性型として、このルフォトレビルの切断型は抗ウイルス機能を持っています。それが、新型コロナウイルス感染症の治療法としての成功の鍵です。幸いなことに、lufotrelvir は複数の変異に直面しても有効性を示しています。これは、SARS-CoV-2 ウイルスの変異を何度も目撃してきたため、貴重な特性です。
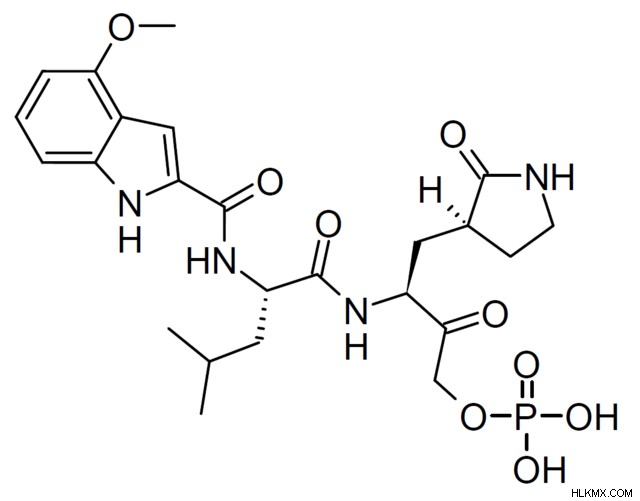 ルフォトレビルの分子構造。ニルマトレルビルがシアノ基を有するところにリン酸基が存在することがわかります。
ルフォトレビルの分子構造。ニルマトレルビルがシアノ基を有するところにリン酸基が存在することがわかります。 もともと、ルフォトトレルビルはエピマー化する傾向があるため、安定性に欠けていました。 エピマー間の相互変換 (1 つの異なるキラル中心を持つジアステレオマー)は、分子の生物活性、代謝、および分解に抵抗する能力に影響を与える可能性があります。ルフォトレビルの場合、分解する傾向が特に顕著な問題でした。これを改善するために、製薬学者は医薬品開発プロセス中にルフォトレルビルを改変しました。このような修飾には、クライゼン付加 (炭素-炭素結合を形成して分子を延長する) やリン酸化 (リン酸基を生成する) などがあります。明らかに、これらの変更にはそれだけの価値がありました。臨床研究では、プロドラッグがほぼ完了して活性型に変換されることが示されています。有効な薬剤の割合が多くなると、その薬剤を生み出した高価で時間のかかる薬剤開発の努力が最大限に活用されるため、その薬剤はより効率的になります。
ルフォトレビルの活性型への切断は血流中で起こることに注意してください。これは、ルフォトレビルが静脈内、血流に直接投与されるという事実によって促進されます。ルフォトトレビルの活性型が効果を発揮すると、体はアミド加水分解によって薬物を除去します。この代謝プロセスについては、今後さらに詳しく説明します。これまでのところ、新型コロナウイルス感染症の治療薬が体内に入るとどうなるかについて多くのことを学んできました。次に、一歩下がって、私たちがほのめかしたトピック、つまり、そもそもそれらの薬がどのように体内に入るのかを検討します。
ドラッグデリバリーの複雑さ
ニルマトレルビルとその前駆体分子ルフォトレルビルは密接に関連していますが、いくつかの大きな違いがあります。これら 2 つの薬剤のうち、ニルマトレルビル (リトナビルという化合物を併用する場合) は、錠剤として投与できるため、一般に好ましい治療選択肢です。対照的に、lufotrelvir は静脈内にのみ投与できるため、代替手段としてはあまり便利ではありません。
患者が薬をどのように摂取するかが重要です。錠剤は持ち運びが可能で、すでに適切な用量に分割されており、医療提供者 (HCP) の立ち会いなしで患者が各回分を服用できるため、患者にとって便利です。利便性は、患者の観点だけでなく医療従事者の観点からも、医薬品において非常に望ましい特徴です。都合がよければ、患者は薬の服用を最後までやり遂げ、処方されたとおりに正確に服用する可能性が高くなります。結局のところ、患者がその薬を適切に使用せず、その効果を享受できない場合、薬を処方することは患者にとっても医療従事者にとっても時間の価値がありません。
錠剤の主な欠点は、効果が現れるまでに時間がかかることです。錠剤を経口摂取すると、錠剤は消化器系を通過し、胃酸によって分解され、腸で吸収されます。このプロセスは患者の観点からは簡単ですが、時間がかかります。副産物として、薬物の化合物が生化学的に分解されます。その方法を見てみましょう。
生物学的利用能と薬物の安定性
消化器系のあらゆる場面で、これらの化合物は酵素などの消化剤と遭遇し、相互作用します。これらの酵素は、化学反応や代謝機能を通じて化合物の化学構造上の官能基を変更し、生物医学研究者の意図から逸脱してしまう可能性があります。体が薬を吸収する前にこれが起こると、薬の全体的な効果が低くなります。 (食事の有無に関係なく錠剤を服用するように言われたことがあるなら、これが理由の 1 つです。胃の中に食物があるかどうかに応じて、体は一部の薬の吸収をより効果的にしたり、より効果的に吸収したりする可能性があります。)ヘルスケアの文脈に置き換えると、これらの状況は、患者が経験する治療効果が少なくなる可能性があります。
逆に、静脈内薬は血流に直接送達され、その効果は錠剤よりもはるかに早く現れます。静脈内投薬は消化プロセスを完全に省略するため、完全な生物学的利用能を示します。 バイオアベイラビリティ 循環系に到達する薬剤の割合を測定するため、静脈内薬剤の(理論上の)バイオアベイラビリティは 100% になります。消化プロセスのおかげで、薬物の一部が体の代謝で常に失われるため、錠剤の生体利用効率は低くなります。科学者は、薬の持続期間の指標としてバイオアベイラビリティを測定します。バイオアベイラビリティが高いと、患者は、バイオアベイラビリティが低い薬剤と比較して、単回投与の効果がより長く持続すると感じます。したがって、薬の投与方法によって、患者がそれをどのように経験するか、またその期間に違いが生じます。バイオアベイラビリティなどの標準化された測定値を使用すると、研究者が非常に多様な薬剤間で公正な比較を行うことができるため、会話がさらに深まります。
薬剤が錠剤と静脈内投与の両方の形式で利用できる場合、それぞれの形式で異なる用量が使用されます。これにより、フォーマットのバイオアベイラビリティの違いが補われます。今では、薬が錠剤の場合、循環器系に到達できる薬の量が少なくなることがわかっています。薬が錠剤として送達される場合、静脈内に送達される場合と比較して、より高い用量で送達されます。ここで、バイオアベイラビリティが薬物の送達形式、用量レベル、投与量などの要因に直接関係していることは明らかです。
他にも微妙な要因が関係していることにも留意してください。たとえば、研究者は、患者集団の中で、各患者に薬物が吸収される速度と量には個人差があることに気づきました。研究者は、薬物の吸収が、薬物を摂取する時間帯、患者の体重、生物学的性別などの要素に依存することをある程度理解しています。しかし、研究者は医薬品を設計する際、吸収に影響を与える可能性のあるさまざまな特異性のすべてを完全に説明することはできません。代わりに、安全で、予測可能で、可能な限り効果的な方法で、大多数の患者に効果がある薬を設計することに努めています。
これらすべての考慮事項は、医薬品の安定性に関する会話を豊かにします。医薬品では安定性が重要です。 医薬品が製造されてから患者が使用するまで一貫した特性を維持する能力を指します。薬物の安定性の評価は、患者の体の内部と外部の両方で継続的に行われます。たとえば、製薬研究者は、医薬品が長期保存可能であり、使用期限までその品質と有効性が確実に維持され、服用後に患者の健康に有意義な影響を与えることを保証したいと考えています。安定性が低いということは、薬が意図した期間にわたって意図したとおりに機能しないことを示します。これは、明らかに薬が適切に効くことを期待している患者にとって深刻な影響を与える可能性があります。
酸化と加水分解の差し迫った脅威
薬物の安定性を日常的に脅かす化学反応の 2 つの例は、酸化と加水分解です。 酸化 薬剤が光や熱などの条件にさらされると、時間の経過とともに電子が失われる反応が起こる可能性があります。劣化を防ぐために、メーカーは医薬品の保管について、どのような温度範囲で、どの程度光から保護するかなど、具体的な指示を提供しています。どれだけの化学反応が、化合物が他の分子の電子をどのように盗み、交換し、失い、獲得するかによって左右されることを考えてみてください。不適切な保管条件により酸化が早まってしまうと、薬物の化学構造の電子数が本来のものとは異なるため、通常の方法ではそのような反応が起こりません。場合によっては、これにより薬自体が本来の効果を発揮できなくなる可能性があります。
製薬メーカーの保管指示に従うだけで、酸化の可能性を最小限に抑えることができます。しかし、酸化以外に、より一般的に観察される薬物の分解経路は加水分解です。 加水分解 分子の化学結合を切断するために水を使用することが含まれます。分子の開始構造によっては、単純な加水分解反応でその生化学的プロファイルが完全に変化する可能性があります。水の存在下では、医薬品によく見られる官能基(エステルやアミドなど)がカルボン酸基やアルコール基に変換される可能性があります。
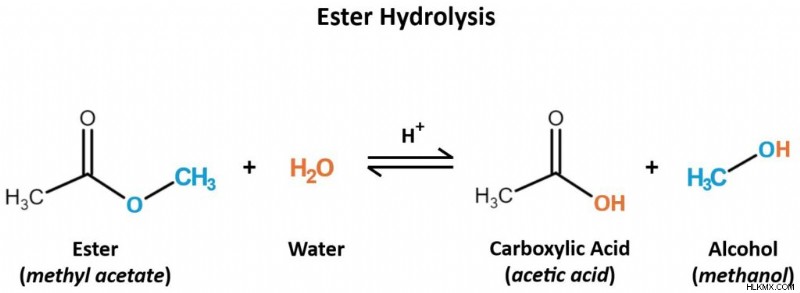 酸性条件下では、水分子がエステル分子をカルボン酸とアルコール生成物に加水分解します。これは可逆的な反応ですが、薬の機能を妨げる可能性があります。
酸性条件下では、水分子がエステル分子をカルボン酸とアルコール生成物に加水分解します。これは可逆的な反応ですが、薬の機能を妨げる可能性があります。 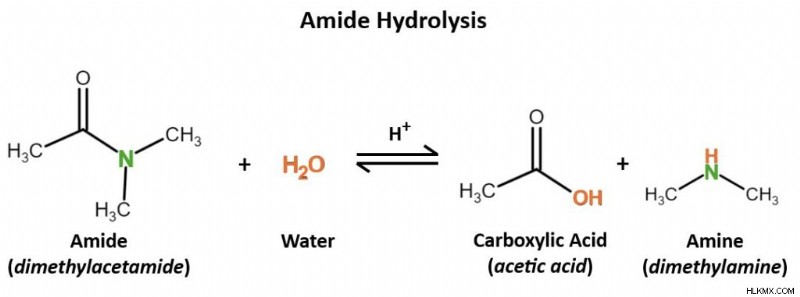 水は、再び酸性条件下でアミドを加水分解し、カルボン酸とアミン生成物を生成します。
水は、再び酸性条件下でアミドを加水分解し、カルボン酸とアミン生成物を生成します。 体内では、さまざまな組織に存在する酵素のおかげで加水分解が起こります。これらの酵素が薬物を加水分解する速度が速ければ速いほど、その薬物の効果の持続時間は短くなります。非加水分解薬と同じ効果を得るためには、より頻繁に、またはより高い用量が必要になる場合があります。したがって、薬の有効性を高める 1 つの方法は、そもそも加水分解しにくい官能基を使用して薬を設計することです。
それにもかかわらず、薬が化学反応を起こすという事実は本質的に悪いことではありません。結局のところ、薬は最終的に分解する必要があります。そうしないと、薬物レベルが体内に蓄積し続け、患者は毒性や臓器損傷などの不快な副作用に苦しむ可能性があります。重要なのは、研究者が薬物代謝の微妙なバランスをどのようにとるかということです。理想的には、薬剤は患者の体内で治療効果を発揮するのに十分な期間、早期の化学反応に耐えるべきです。これらの効果が完了すると、代謝化学反応に屈して体から排出できるようになります。この代謝がいつ起こるべきかを正確に特定することは、 研究者が生体内で薬剤を研究する薬剤開発段階における中心的な問題です。 体の活性酵素、化合物、組織の間でそれがどのように機能するかを理解するため。
この記事で紹介した新型コロナウイルス感染症治療薬は、それぞれの固有の特性に関係なく、抗ウイルス薬として機能します。 (追記: 確実に見分ける方法は、それぞれの名前の末尾に「-vir」があることです。) しかし、これら 4 つの化合物のうち 1 つは他の化合物とは異なります。リトナビルは単なる抗ウイルス薬ではありません。それは抗レトロウイルス薬です。 。これが新型コロナウイルス感染症 (COVID-19) の文脈で何を意味するのか考えてみましょう。
バックアップ:レトロウイルスとは何ですか?
抗ウイルス薬は 1 つ以上のウイルスを標的としますが、 抗レトロウイルス薬は特にレトロウイルスを標的とします。 。宿主細胞に感染すると、 レトロウイルスは逆転写酵素を使用します。 酵素を利用して、自身の RNA ゲノムに相補的な DNA 鎖を作成します。生物学のセントラルドグマでは、DNA は RNA に転写され、最終的にはタンパク質が生成されると述べていることを思い出してください。 RNA から DNA を作るということは、典型的な転写プロセスを逆転させることを意味します。この RNA から DNA への配列が、レトロウイルスの名前の由来です。レトロウイルスは、その遺伝物質が DNA に変換されると、宿主細胞の自然な複製機構を引き継ぐことができます。これにより、レトロウイルスはゲノムを複製し、それ自体の新しいコピーを作成して感染を伝播することができます。おそらく、レトロウイルスの最もよく知られた例は、HIV/AIDS の背後にあるウイルスである HIV-1 でしょう。
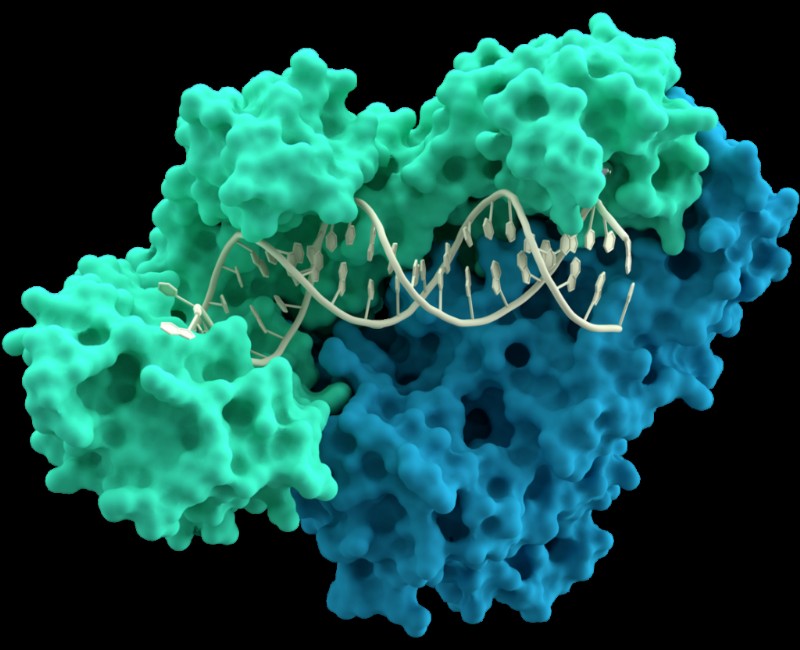 DNA 分子と相互作用する逆転写酵素の p66 (緑色) および p51 (青色) サブユニットのモデル (中央)。
DNA 分子と相互作用する逆転写酵素の p66 (緑色) および p51 (青色) サブユニットのモデル (中央)。 SARS-CoV-2 などのコロナウイルスはレトロウイルスではないことに注意することが重要です。コロナウイルスとレトロウイルスは、完全に異なる分類科に属します。もしそうなら、なぜリトナビルのような抗レトロウイルス化合物がコロナウイルスと戦うのに役立つのでしょうか?
違いはあるものの、レトロウイルスとコロナウイルスの間には重要な類似点がいくつかあります。どちらも RNA を遺伝物質として使用し、宿主細胞の生来のメカニズムを乗っ取って自己複製し、複製にはプロテアーゼを必要とします。 プロテアーゼ タンパク質を分解する酵素です。この場合、レトロウイルスまたはコロナウイルスが増殖するために必要なタンパク質を分解します。
ニルマトレルビルとリトナビル、そしてルフォトレルビルはすべてプロテアーゼ阻害剤です。 。その目的は、レトロウイルスやコロナウイルスの拡散を助けるプロテアーゼ酵素を阻止することです。リトナビルは実際には HIV-1 治療薬として始まりました。新型コロナウイルス感染症(COVID-19)のパンデミック中、科学者らはリトナビルを再利用して、SARS-CoV-2に対するその影響を研究した。それで、おい、それは影響を与えたのだろうか。
身体は、特に腸と肝臓で、時間の経過とともにプロテアーゼ阻害剤を自然に代謝します。薬学的観点から見ると、これはプロテアーゼ阻害剤が必然的に分解されることを意味します。これらの薬を体内でより長く持続させるために、この代謝を遅くする別の薬を投与することができます。パクスロビッドの主人公であるニルマトレルビルが、単一の薬剤としてリトナビルを併用しているのはこのためです。どちらもプロテアーゼ阻害剤ですが、リトナビルはプロテアーゼ阻害剤を分解する CYP3A4 酵素を阻害するように特別に配合されています。言い換えれば、リトナビルはニルマトレルビルを代謝する力を遅くし、ニルマトレルビルが体に長く影響を与えることを可能にします。代謝の脅威が軽減されたため、ニルマトレルビルは、新型コロナウイルス感染症の蔓延を可能にするタンパク質の分解という、本来の役割に集中することができます。
薬物の再利用は試行錯誤の繰り返しになりがちです。研究者は、対象の病気についてすでにわかっていることを利用して、既存のどの薬がその病気に対して効果があるかを予測します。次に、研究室の設定や臨床試験で、 その薬が実際にどの程度効果があるかをテストします。 対象の病気に対して効果があります。臨床試験が成功した場合、規制当局はその病気の治療薬を承認する可能性があります。
薬が効かない場合はどうでしょうか 仕事?
薬が市場に投入されると、研究室や臨床研究の枠を超えて、その薬が実際にどの程度効果があるかを確認できるようになります。場合によっては、薬がまったく問題なく意図したとおりに機能することがあります。ただし、計画どおりに物事が進まず、薬が実際の患者に届いて初めて新たなハードルが現れることもあります。
これを現代の最大の医学的脅威の 1 つである抗生物質耐性の観点から見てみましょう。 抵抗 これは、薬の標的となる病原体(この場合は病気の原因となる細菌)が徐々にその薬(抗生物質)に耐えられるようになるという意味です。 This has dire implications for the pharmaceutical industry, which then must devise a new bacteria-killing drug that the bacteria aren’t resistant to yet, and for the patients who suffer from incurable bacterial infections in the meantime.
Unfortunately, this phenomenon happens with protease inhibitors, too. Viruses that are normally susceptible to protease inhibitors can, over time, develop resistance to those drugs. When that happens, the protease inhibitors become less effective as antiviral medications. How does this happen in the first place?
In order to stop viral replication, a protease inhibitor must bind to a specific site on the virus’s protease. This is how protease inhibitors work under normal circumstances, as intended, to treat a viral infection. In its genome, a virus encodes the proteases that it needs for replication. But, as we know, genetic material can mutate — and any mutation can change the nature of the protease.
If a mutation changes the protease’s active site, this directly impacts its affinity for binding to the protease inhibitor. It’s possible for the active site to mutate to have a lower affinity for the drug, which limits the medication’s ability to target the protease. This is how protease inhibitor resistance arises. Without a selective target available, the protease inhibitor can’t do its job effectively, so it’s no longer a useful solution against the virus it ought to fight.
Mutations can happen spontaneously, and they tend to arise as a virus evolves over many replication cycles. This introduces a bit of a conundrum:scientists invented protease inhibitors to prevent viral reproduction, but as a result of viral reproduction itself, mutations can arise that change a protease inhibitor’s effectiveness. During the COVID-19 pandemic, we saw precisely how concerning viral evolution and mutation are, as newly-evolved mutant variants repeatedly rendered our vaccines less effective.
To overcome the challenging prospect of a protease-inhibitor–resistant virus, protease inhibitors can be used in combination with antiviral medications that have different targets. This way, even if the virus’s active site mutates to become resistant and the protease inhibitor can no longer bind there, another medication can step in to target a different structure or function of the virus instead. Spreading the virus-fighting burden across multiple diverse drug classes can help stop the virus’s spread. But wait — what’s a drug class, and what does it mean for the virus that causes COVID-19?
Class is in Session:Pinpointing the Right Medication for the Right Job
There’s no “miracle” antiviral drug that can treat every viral disease out there, but that doesn’t stop scientists from trying! Researchers group similar medications into classes based on their properties and functions. Oftentimes, these classes directly describe how the drug functions. Some familiar examples readily come to mind:drugs in the stimulant class stimulate the body or mind, contrasted with drugs of the depressant class that reduce arousal, while analgesic drugs relieve pain (the word “analgesic” comes from Greek roots that mean “without pain”).
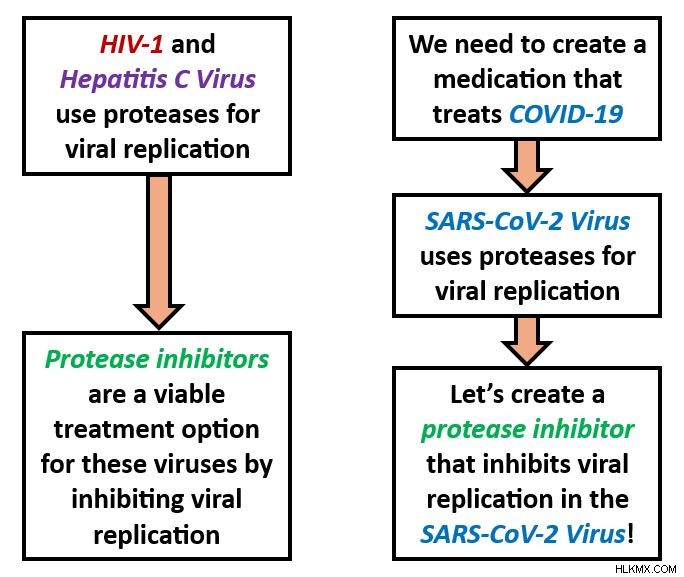
Protease inhibitors are another class of drugs that do exactly what their name implies. By inhibiting proteases, a type of enzyme that SARS-CoV-2 particles use for reproduction, protease inhibitors interrupt the viral life cycle by preventing the virus from replicating. The virus must make many copies of itself to infect new host cells, so preventing viral replication prevents the spread of COVID-19.
Researchers already applied the same concept to fighting the viruses behind HIV/AIDS and hepatitis C. Understanding the commonalities within a particular drug class makes it easy to translate existing medications into new contexts to treat different diseases. To devise an effective antiviral medication to treat COVID-19, researchers had to understand a few simple, yet essential, points. First, they learned that the SARS-CoV-2 virus uses proteases in its replication process. Second, they knew that the viruses that cause AIDS and hepatitis C also use proteases to reproduce. Third, protease inhibitors already existed as safe, effective medications for treating HIV/AIDS and hepatitis C.
From here, scientists could apply this logic in a straightforward way in order to conclude that protease inhibitors are a viable COVID-19 treatment option. If protease inhibitor drugs are already known to work against other viruses that replicate via proteases, and SARS-CoV-2 is known to replicate via proteases too, why not pursue a protease inhibitor as a COVID-19 drug?
 During drug discovery, biomedical researchers don’t always have to start from scratch. Instead, they may be able to build upon existing knowledge of which medications work well against pathogens of similar diseases. Inspired by existing drugs for HIV and hepatitis C, these logical reflections guided researchers to develop protease inhibitors for SARS-CoV-2.
During drug discovery, biomedical researchers don’t always have to start from scratch. Instead, they may be able to build upon existing knowledge of which medications work well against pathogens of similar diseases. Inspired by existing drugs for HIV and hepatitis C, these logical reflections guided researchers to develop protease inhibitors for SARS-CoV-2. In some ways, drug discovery is a very sensible process. But in practice, there are a lot of factors that threaten to get impede what ought to be a smooth, uncomplicated approach. Let’s take a look.
Challenges in Treating COVID-19
Pandemics are among the most urgent public health scenarios; time is truly of the essence. To conquer the crisis, medical experts must develop and distribute a cure faster than the disease is spreading. But we know the SARS-CoV-2 virus causes COVID-19, and viral diseases, in general, cannot be cured — only managed or treated.
Facing an incurable disease, how can we devise an effective treatment, and fast? Taking on this challenge meant overcoming SARS-CoV-2’s natural evasive characteristics, drug development roadblocks, and sociocultural factors that shaped how people interacted with COVID-19. To understand why these details had such a key impact on the pandemic, let’s evaluate them in greater depth.
Virology 101:How Viruses Evade Our Efforts to Eradicate Them
We know how to take control of stubborn viruses because we’ve managed to do it many times before. For example, you’ve likely sustained a barrage of vaccines for viral diseases like chickenpox, measles, and polio. And everyone can recite by heart the cardinal rules of flu season — stay home when you’re sick, cover your mouth when you cough and sneeze, and wash your hands often. Public health principles like these are somewhat of a tradition, and we know these rules of how to beat disease. So, what happens when we encounter a virus that doesn’t play by the rules?
What makes an effective antiviral medication?
Viruses have certain properties that can make them more difficult to target than pathogens like bacteria or parasites. First of all, there’s an ongoing scientific debate as to whether viruses are living or nonliving. Viruses have their own genetic material and, inside of a host cell, they exhibit some characteristics of life, like the ability to reproduce (viral replication )。 However, viruses can’t function independently, and therefore can’t do much damage, without the help of a living host cell. Since they need living hosts’ support to execute their functions, many scientists view viruses, in and of themselves, as nonliving. This invites a unique conundrum:If something isn’t alive, is it actually possible to use medications to kill it?
As part of the drug discovery process, pharmaceutical researchers determine how their medication will impact its target (which might be a protein, antibody, gene, virus, bacterium, etc.). Many drugs work by impacting the target’s ability to function, but this might not be useful against viruses. For example, a drug that works by interfering with the target’s metabolism wouldn’t be an effective antiviral drug because viruses don’t have their own metabolic processes.
Living or not, we know that viruses are vulnerable to antiviral medications. Strong antiviral medications account for their target’s normal mechanisms and viral load. By closely studying those mechanisms — how the virus infects and moves through the body, infects healthy host cells, replicates its genetic material, and causes physical symptoms — scientists can pursue a drug that interferes with them.
Viral load refers to how much virus is present in a patient’s blood. Viral load can change over the course of an infection, and it can indicate how sick the patient is. For certain diseases, a higher viral load indicates that the patient is more contagious. Some antiviral medications are intended to reduce viral load, alleviating the patient’s infection and protecting other people from catching it. (In this way, reducing viral load is a goal of a long-term HIV treatment called antiretroviral therapy , or ART .)
What’s the Password?:How Viruses Enter Host Cells
Viruses are among the smallest biological agents. After all, they have to be, in order to penetrate host cells. Viruses usually enter host cells through receptor-mediated endocytosis , a process by which the viral particle binds to a receptor on the cell membrane and passes into the cell. When descending upon a new host cell, the virus hunts for specific receptors that will bind to proteins on its own membrane.
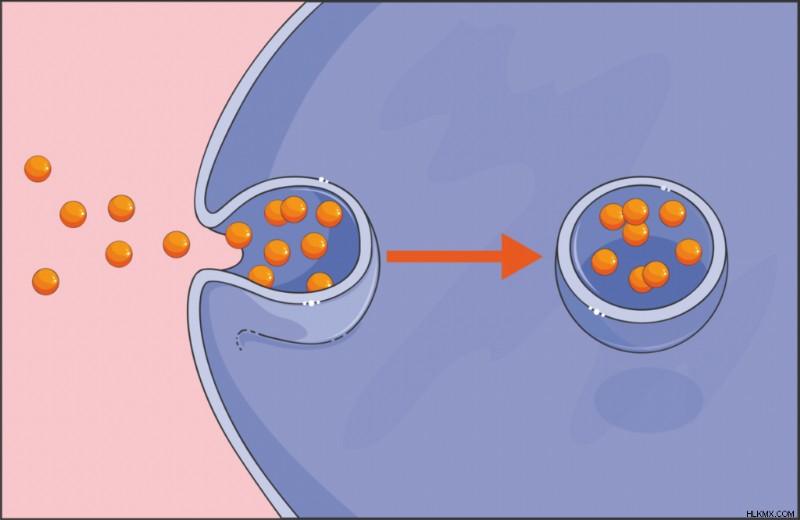 Endocytosis is a process by which particles can enter a cell. Viruses use this tactic to bind to a host cell’s membrane and invade the cell.
Endocytosis is a process by which particles can enter a cell. Viruses use this tactic to bind to a host cell’s membrane and invade the cell. This penetrative mechanism is sometimes what an antiviral drug targets. A drug that interferes with this protein’s binding to a membrane receptor prevents the virus from reaching host cells. Researchers extended this strategy to COVID-19 vaccines that notably target SARS-CoV-2’s spike protein , which binds to host cells’ ACE2 receptors. All coronaviruses have spike proteins, but the protein’s chemical makeup can fluctuate across different viral variants. This is why scientists continuously produced COVID-19 vaccines:each new version of the vaccine targeted the spike protein’s latest disguise. We already knew about coronaviruses before COVID-19 happened, but developing a COVID-19 medication required learning about the special intricacies of SARS-CoV-2’s spike protein in particular.
For being such tiny agents, viruses sure put up a big fight. A drug spurs the body to act upon a virus, but this could inadvertently lay the groundwork for further harm. In order to damage viruses, antiviral treatments must also damage the host cells that those viruses occupy. This can have further implications for the health of the patient or the symptoms that they experience. Therefore, antiviral treatments represent a balancing act, selective toxicity , between destroying the virus and preserving the patient’s own tissues.
Unfortunately, there’s no easy solution to this dilemma. Any step in the viral life cycle would be a good target for an antiviral drug, but the host cell would probably also suffer. Some antivirals reduce the risk to the patient’s health by targeting a virus-specific molecule or behavior, leaving the host cells relatively untouched. That’s the inspiration behind COVID-19 drugs like nirmatrelvir/ritonavir. Nirmatrelvir/ritonavir inhibits a protease that SARS-CoV-2 uses for replication, which prevents the virus from reproducing. (Other COVID-19 medications, like remdesivir , disrupt the replication process by introducing steric hindrance as the virus replicates its RNA. This steric hindrance stands in the way of RNA replicating to completion, putting a pause in the viral life cycle and the SARS-CoV-2 virus at a loss.)
With antiviral drugs, researchers must weigh the benefit of weakening the virus against the risk of weakening host cells. An antiviral medication that preserves a patient’s infected cells would be an ingenious discovery and a very promising treatment option — something to consider next time you find yourself bored in the lab!
Playing the Long Game
Recall from our previous article that public health professionals use epidemiological surveillance to track disease outbreaks on a population scale. We can extend this concept to a much smaller scale:detecting microscopic viruses within the body. Their minute size isn’t the only characteristic that can make viruses hard to detect. Some viruses are pros at staying inconspicuous for extended periods of time. During these periods, the virus in question may not cause obvious symptoms (or if so, the symptoms may be nonspecific). It may even fail to appear on test results.
Sometimes observed in viral infections like HIV, Epstein-Barr virus, and hepatitis, this phenomenon is a latency 期間。 Latency periods happen when the virus is dormant for spans of weeks, months, years, or even decades. Dormancy means that the virus has infected a host, but isn’t actively replicating, or it’s replicating very slowly. Remember, for the infection to spread within the body, or from an infected to healthy person, the virus must replicate. The act of replication kills the host cell. Then, in the aftermath of cell death, the progeny from that replication seek new host cells and spread the infection.
Although certain viruses share some resemblances, like these particular viruses’ ability to stay surreptitious for long-term periods, viruses overall demonstrate very diverse features. For instance, SARS-CoV-2’s genome is composed of RNA, but many viruses’ genomes are made from DNA just like ours. Different viruses also boast different physical properties, replication techniques, and thrive in a range of environmental conditions. Maybe you can’t disrupt the virus’s life cycle, but can you do something to make its environmental conditions less hospitable? In light of such diverse traits, making antiviral medicines might seem like a fruitless pursuit, but keep in mind that every new trait presents a new angle to attach the virus.
Identifying a given virus’s individual idiosyncrasies helps researchers tailor a medication perfectly to that virus — but also means that most antiviral medications can only treat one or a handful of viruses. This lies in stark contrast to broad-spectrum antibiotics , which target numerous bacterial species. Not all antibiotics are broad-spectrum, but this all-encompassing quality is hard to replicate in antiviral drugs. Broad-spectrum antivirals do exist, but because viruses evolve so rapidly, the best antivirals would be able to defeat multiple existing strains while anticipating future variants, which is essentially a guessing game. A good place to start is with antivirals that target entire families of viruses, like coronaviruses or herpesviruses for example, that attack a stable characteristic which all of the family members have in common. Yet another example of how the shared features among different pathogens serve as the groundwork for building a single drug that fights all of them!
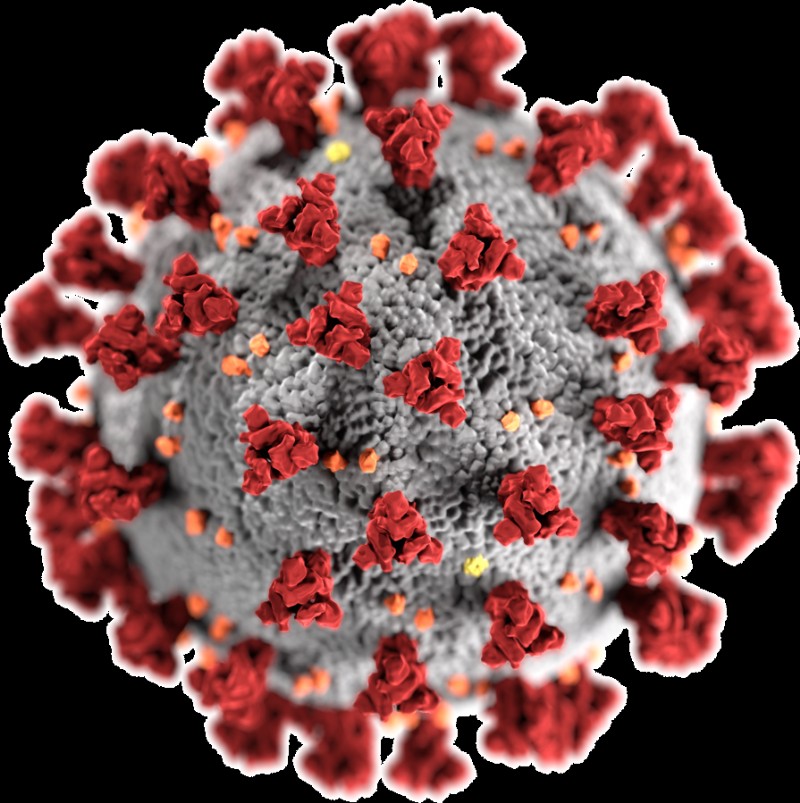 Spike proteins (red) on a SARS-CoV-2 particle project outward to readily bind with ACE2 receptors on a host cell’s membrane.
Spike proteins (red) on a SARS-CoV-2 particle project outward to readily bind with ACE2 receptors on a host cell’s membrane. Ready, Aim, Fire! All about Drug Targets
Earlier, we discussed how protease inhibitors bind with proteases that the SARS-CoV-2, HIV-1, and hepatitis C viruses encode. Recall that this binding happens selectively, and directly leads to the inhibition of viral replication. In pharmaceutical terms, we describe this dynamic dance as the protease inhibitor targeting a particular binding site on the protease. Alternatively, we can say that the protease (more specifically, the binding site) is the target of the protease inhibitor medication. But why do medications need to have targets at all?
Drugs with Multiple Targets
Most drugs need specific targets in order to treat a particular condition. But there are indeed some drugs, like certain anti-inflammatory medications and chemotherapy treatments, that target the body as a whole. This broad approach, polypharmacology , involves one drug affecting multiple targets. Anti-inflammatory drugs reduce inflammation by acting on prostaglandins — lipids that are present all over the body. And just think of the vast array of side effects that accompany chemotherapy (fatigue, nausea, hair loss, and more). The fact a single drug causes side effects that are so different from one another, which impact different systems within the body, indicates that the drug is acting on several distinct targets.
Considering the meticulous effort that goes into seeking and identifying precise targets during the drug discovery process, it might sound surprising that scientists purposely design some medications to have many targets. But for diseases such as cancer, whose wide-ranging warpaths can span multiple organs and pose a risk to the body overall, having a less specific set of targets might be the ideal solution. Each affected organ is unique, with its own profile of cell types, enzymes, and functions. The goal here is to give patients a better chance of beating a whole-body disease with a drug whose targets live throughout the whole body.
Depending on the nature of the disease, a drug’s ability to target many molecules may be either advantageous or disadvantageous.
Drugs with One Target
Let’s face it:it’s hard to maintain this big-picture outlook when working with such tiny molecules! We saw from the protease inhibitor discussion that a single binding site in the target (and sometimes a single mutation within a single binding site) can make all the difference as to whether a medication flourishes or flounders. What muddles this problem even further is the fact that a target can have multiple domains that serve as binding sites, or two very different types of molecules could have similar binding sites that interact with the drug. How do pharmaceutical researchers make a drug that acts on one binding site of interest, while ignoring all the others?
For drugs that target only one molecule, the binding interactions between the medication and its target are extremely specific. That’s an understatement! This high specificity minimizes the risk of off-target effects that can have unpleasant or dangerous consequences on the patient’s health. Designing an effective drug that has one, and only one, target requires a deep understanding of binding affinity and the structural qualities that govern it.
Remember that the drug and the target each boast a chemical structure that’s full of functional groups. Each functional group has distinctive properties that influence its reactivity, behavior, and interactions with other molecules. This means that structural characteristics lie at the core of the drug-target binding, and therefore at the core of drug effectiveness. By manipulating the functional groups in the drug’s molecular backbone, researchers can manipulate the reactions that the drug undergoes, as well as its propensity to bond with a specific domain on the target. It’s astonishing that changing out even one little atom could introduce a different a functional group and, by extension, impact a medication’s ability to work properly! Even if the drug’s functional groups stay the same, a minor change in their spatial arrangement might completely change the medication’s function.
Consider enantiomers :molecules whose structures are mirror images. One notorious case of this chirality making or breaking a medication is thalidomide. Thalidomide is a drug that was originally marketed as a morning sickness remedy. It exists as two enantiomers:the R enantiomer has a sedative effect that alleviates symptoms like morning sickness, while the S enantiomer can cause birth defects. The only chemical difference between these two drastically different outcomes is how these molecules’ atoms are spatially arranged. To make matters worse, thalidomide can interconvert its enantiomers in vivo , so even if a patient were only administered the relatively harmless R enantiomer, the teratogenic S enantiomer may arise in the body afterwards. By contrast, medications that only exist as one enantiomer, as opposed to a racemic mixture, are enantiopure drugs.
Another example of a more-than-microscopic structural change having a larger-than-life impact is the methamphetamine molecule. Methamphetamine is a stimulant and recreational drug, with side effects like vasoconstriction and rapid breathing. Its optical isomer levmetamfetamine, meanwhile, serves as a nasal decongestant of all things! Again, we see that one small switch in these drug molecules’ atomic arrangements leads to wildly different health effects.
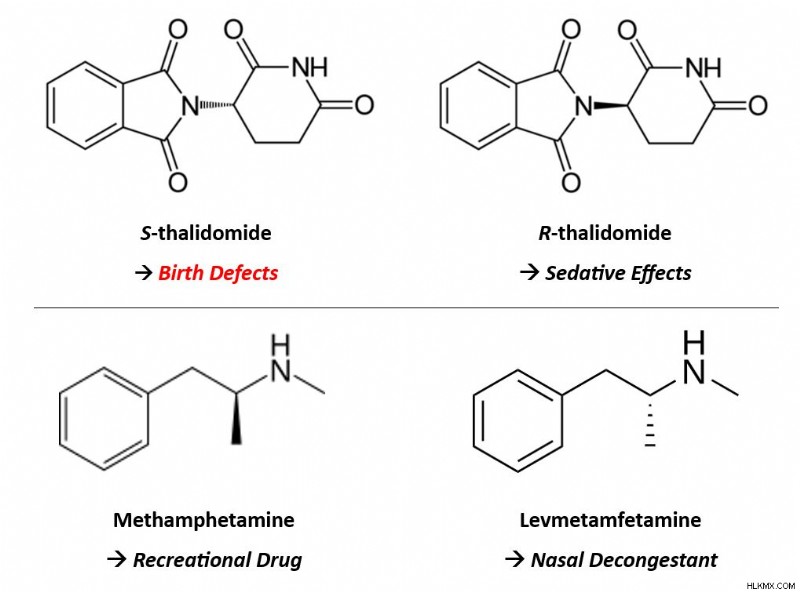 Though the only difference between each of these sets of enantiomers is the spatial arrangement of their atoms, their ensuing medical effects differ greatly.
Though the only difference between each of these sets of enantiomers is the spatial arrangement of their atoms, their ensuing medical effects differ greatly. A recurring notion in drug development is that medications are intended to be as safe and effective as possible. However, no medication can be 100% safe nor 100% effective. No matter what, there’s always the risk of side effects, off-target effects, and unwanted interactions. Regardless, scientists can maximize safety and effectiveness by tailoring a drug’s chemical properties, like its structure and functional groups, to be as specific as possible to the target of interest.
Unfortunately, achieving that specificity can be an intense challenge, especially when only one target is desired. But when different pathogens employ the same biochemical processes or enzymes as each other — like how SARS-CoV-2, HIV-1, and hepatitis C virus all employ proteases for replication — these features serve as a good starting point for drug design. Could that common feature potentially function as the drug’s target? And since several pathogens share that feature, could the drug therefore be effective against all of the pathogens? For viruses in particular, all viruses must replicate because replication is the only way viral diseases can spread to new hosts. That’s why popular COVID-19 medications target molecules, like proteases, that have a central role in SARS-CoV-2 replication. (The same is true for the protease inhibitor drugs that treat HIV and hepatitis C infection.)
Here, we’ve seen that slight changes in the drug molecule yield big impacts on its ability to bind selectively with its target (or targets). Later, we’ll talk about another highly-specific mechanism in combating disease:the interactions between antibodies and antigens. For now, let’s dive into the question of why COVID-19 medications were unusually difficult to make.
Drug Development under Dire Circumstances
The small but significant principles that we’ve mentioned so far — the fact that antibiotics don’t work against viruses, the puzzle of creating a new medication based on clues from existing ones, the arduous task of designing a drug with meaningful targets — only complicated the hunt for efficacious COVID-19 medications. Numerous additional factors were already at play, presenting challenges for drug development during a time when we needed it most.
Some of these challenges ran deep. Hardening travel restrictions and heightened political tensions, for example, strained the pharmaceutical supply chain at its core. Patients often rely on drugs manufactured elsewhere in the world, but temporary limits on international travel jeopardized typical medication supply. Worth noting is that most active pharmaceutical ingredients (APIs ), the component of a drug that gives it its therapeutic effect, are manufactured outside of the U.S. This includes being manufactured in countries that the pandemic hit hard, such as China. Importing drugs and APIs — and exporting American medicines to patients around the world — normally happens in a steady stream that ensures patients everywhere can receive their treatments when they expect to. With the short-term closures of pharmaceutical facilities and chemical plants domestically and abroad, this promise went unfulfilled in many cases. Even a brief pause in drug manufacturing can ripple into long-lasting consequences for patients.
 Pandemic-related travel restrictions hindered international drug distribution, preventing some medicines from reaching patients when expected.
Pandemic-related travel restrictions hindered international drug distribution, preventing some medicines from reaching patients when expected. Other points in the drug development process were interrupted, too. The Food and Drug Administration (FDA ), the American pharmaceutical regulatory agency, also monitors pharmaceutical sites in foreign countries. These inspections confirm that U.S.-bound drugs comply with the same rigorous safety and quality standards as those made in America. International travel restrictions, again, delayed these investigations. Inspections must happen before any medications get distributed, so from a patient perspective, postponed inspections equates to postponed treatment.
The COVID-19 pandemic struck all steps in the pharmaceutical supply chain:manufacturing, production, approval, distribution, and everything in between. This highlighted glaring vulnerabilities in this industry’s very framework, and those vulnerabilities’ effects on patients. We expect pandemics to arise occasionally, but we can’t predict when, and no two disease outbreaks are the same. That aspect of “unexpectedness” makes it extra hard to accommodate them when they do happen. Even more urgently, it underscores the need to make our drug development processes more resilient against health emergencies like pandemics. Let’s take a moment to see what that impact looks like in the context of pharmaceutical research.
A Logistical Nightmare
As soon as the World Health Organization classed COVID-19 as a pandemic, the clinical research sector scrambled to accommodate this. Mounting concerns over a mysterious disease abruptly brought many clinical trials to an indefinite pause. By the time a clinical trial starts, the researchers have already carefully planned and committed to its study protocol. During COVID-19, social distancing guidelines forced them to reimagine studies in virtual formats when possible, and postpone them when not. Trials that hadn’t begun yet were hit even harder. The number of prospective study participants plummeted as they feared COVID-19 exposure in the medical facilities where trials often occur. Some studies couldn’t even get off the ground, but those that could suddenly found themselves stuck in midair.
What’s the problem with putting a clinical trial on pause? It’s not as simple as picking up where the study left off a few weeks afterward. Surprisingly, a lot can happen in the span of a few weeks. If study participants have already received a trial dose of the drug candidate, they might experience new side effects. Researchers need to monitor these complications closely to document and address them, and to ensure the drug’s safety. Ongoing communication is paramount during trials by ensuring patients understand the nature of the study and can express their concerns. Anything that interferes with these open lines of communication, like a brutal pandemic, potentially puts the patient’s safety at risk.
During this frantic period, coronavirus clinical trials took center stage as new COVID-19 medications, therapeutics, and vaccines evolved. A large portion of biomedical research funding, media attention, and public health efforts were diverted to these studies. There’s nothing inherently bad about this, but COVID-19 wasn’t the only disease that needed trials at the time. Pausing routine studies in favor of COVID-19 trials means neglecting, at least temporarily, patients who have other medical conditions. The timing was unlucky, but other diseases didn’t cease to exist just because the pandemic happened. Striking this balance given a wide pool of patients in need, and redirecting funding appropriately, was a big challenge as COVID-19 cases skyrocketed. It even represents complex bioethical questions:How “worth pursuing” is a particular disease compared to others? Is it even possible to “rank” the value of different diseases? Who gets to determine this value?
Among the most unsettling outcomes of the pandemic is that it brought our health care infrastructure’s flaws to light. Many individuals, especially practitioners and patients who experience the health care system firsthand, were already acutely aware of its shortcomings. But COVID-19 exposed these imperfections and made them impossible to ignore. Already stretched thin, medical staff and facilities didn’t have adequate support or resources during intense waves of COVID-19 variants. Issues surrounding health equity, like overcoming health disparities and ensuring accessibility to drug treatments, became serious problems for some patients. These problems predated COVID-19 and aren’t unique to it, but the pandemic certainly emphasized them. As we determine a path forward in a post-pandemic world, public health experts think deeply about how to solve problems like these, to help everyone pursue their healthiest self.
 Resolving a pandemic extends beyond drug development. Health care personnel, regulatory employees, policymakers, and public health experts each have a key role in coordinating an effective pandemic response.
Resolving a pandemic extends beyond drug development. Health care personnel, regulatory employees, policymakers, and public health experts each have a key role in coordinating an effective pandemic response. The COVID-19 Treatment Toolbox
So far, we’ve covered two types of antiviral COVID-19 medications in detail. That’s not the whole story, though. There are other COVID-19 antiviral drugs too, and pharmaceutical treatments aren’t limited to pills either. In this section, we’ll see how the pandemic employed a multitude of other forms of treatment, even making use of the body’s natural defense mechanisms.
Monoclonal Antibodies
Even when it’s combating an infection like COVID-19, the immune system is a very powerful force. A relentless soldier in the battle for your health, its most intrinsic mission is to protect you, and it’s determined not to give up. To achieve this goal, the immune system utilizes its diverse range of physiological intricacies, some of which researchers don’t fully understand yet. Immunologists do understand the basic mechanism of how it works, though.
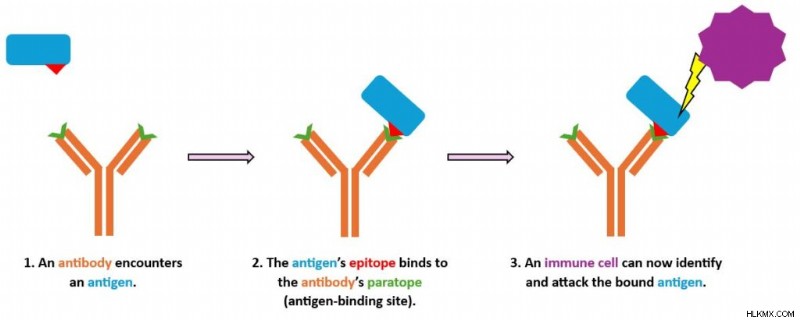
When a foreign pathogen, like the SARS-CoV-2 virus, infects you, we call that pathogen an antigen 。 The immune system recognizes antigens as invaders and mounts an immune response to ambush them. Among other biochemical battalions, it deploys antibodies. Antibodies are proteins made by the body’s B cells that selectively bind to antigens like a key fitting a lock. Binding is a way of flagging the antigen so other immune cells can identify, attack, and neutralize or kill it. As a component in pharmaceutical treatments, antibody therapy is an auspicious option for patients whose bodies can’t mount a sufficient immune response on their own.
How do monoclonal antibodies work?
We can classify antibodies into two broad categories. Monoclonal antibodies (mAbs ) are antibodies that target a single antigen. They’re man-made in the lab by cloning a single lineage of B cells, hence the name. By contrast, polyclonal antibodies (pAbs ) derive from multiple immune cells, arise naturally in the body in response to an infection, and can target multiple antigens.
We usually discuss mAbs as an immunotherapy in the context of cancer, where the “antigen” that they recognize is a protein on the surface of a cancer cell. More recently, their applications have extended to other conditions, including COVID-19. (Another pharmaceutical lingo lesson:a drug whose generic name ends in “-mab” is a type of monoclonal antibody.) When administered to patients, mAbs stimulate the immune system and can improve their chances of fighting off an infection. Creating mAbs in laboratories is an opportunity to precisely tailor them to a specific condition, which can enhance patient outcomes. Pharmaceutical scientists can mass-produce them with high consistency, and off-target effects are relatively unlikely because the mAb binds to only one antigen.
How does that binding make the magic happen? Given its Y-like shape, an antibody has two arms that branch off from its body (the Y’s vertical stem). On the end of each arm is a paratope , the region that binds directly to an antigen. The antigen itself features a region called an epitope 。 The antibody’s paratope and antigen’s epitope are extremely specific to each other. Consequently, the molecules bind together in a selective and precise manner, like a lock and key. Once the antibody has latched on to the antigen, the immune system can take action to attack that antigen.
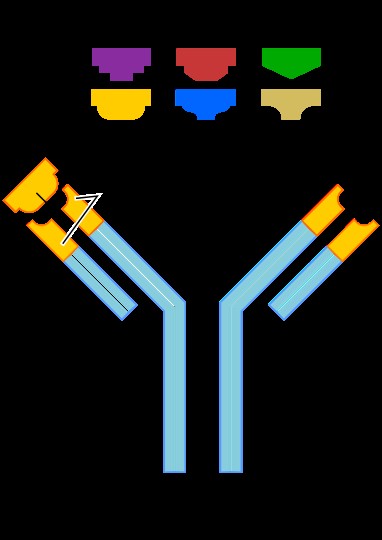 Antigens come in all shapes and sizes, but only a specific antigen can bind to a given antibody’s antigen-binding site (paratope).
Antigens come in all shapes and sizes, but only a specific antigen can bind to a given antibody’s antigen-binding site (paratope). Over time, researchers have found that COVID-19 mAbs can have different levels of effectiveness against certain SARS-CoV-2 variants. COVID-19 mAbs tend to have a harder time fighting off recent variants compared to older ones. As the pandemic evolved, novel variants dominated new infections, and some variants even showed resistance against COVID-19 treatments. It quickly became evident that antibody therapy alone, though a valuable aid, wouldn’t be a long-term solution to COVID-19.
Newly-produced antibodies travel from the B cell (a white blood cell) to the antigen’s location via the patient’s blood plasma. Everyone has blood plasma, but COVID-19 patients may be able to supplement their treatment with convalescent plasma. Next, we’ll see what that means and why it matters.
Convalescent Plasma
We just described how an infection engages the body’s immune response, including increasing the amount of antibodies in the blood. We also mentioned that the immune system’s B cells naturally produce polyclonal antibodies during an infection.
In patients who survive the infection, those antibodies don’t disappear after their symptoms clear up. As the infection resolves, the antigens in the body dwindle. But just in case these antigens dare to show their face around these parts again (in other words, if the patient were to contract the virus again in the future), these antibodies remain in the body, lying in wait to flag them for removal.
Therefore, people who have survived COVID-19 still have COVID-19 antibodies in their blood plasma. Plasma is the part of blood that excludes blood cells and platelets. Survivors can donate this blood plasma, and HCPs then process it and transfuse it into the veins of patients who are actively sick. This was a big deal during the first phase of the pandemic, before researchers managed to make a vaccine that teaches the body’s immune system to create COVID-19 antibodies. And once the vaccines were available, vaccinated folks could donate their antibody-rich plasma to COVID-19 patients even if they’d never actually had an infection themselves.
 Donor blood processing removes components like red blood cells, which is why plasma isn’t red in color.
Donor blood processing removes components like red blood cells, which is why plasma isn’t red in color. Plasma therapy is viable particularly for immunocompromised patients, who may not be capable of launching robust immune responses without it. It’s a great way for COVID-19 survivors to pay it forward and play a personal role in helping current patients. Plasma therapy is useful due to its potential to shorten the duration or severity of infection. In 2020, when no feasible COVID-19 medications were available, having ready-made antibodies in our arsenal was practical and priceless.
Making the Most of COVID-19 Medications
Antibody therapy and plasma therapy are two non-antiviral tools that HCPs relied upon during the worst waves of the pandemic. Once COVID-19 medications hit the market, they became the go-to treatment for active infections because they successfully interrupt the viral life cycle. But if you find yourself infected with COVID-19, the medication that suits your needs might depend on factors like your age and risk of hospitalization. Each of these drugs works most effectively when taken shortly after the onset of symptoms. Why does when you take the medicine matter? It’s ideal to intervene during the initial stages of infection, before the virus has extra time to damage the body. This is especially important in severe cases, when such damage could be extensive.
As is the case with other viral infections, prioritizing rest and fluid intake can go a long way in COVID-19 recovery. In more severe cases, supplemental oxygen and around-the-clock care might be necessary to help hospitalized patients heal. Without innovative antivirals around yet, early waves of the pandemic relied heavily on supportive care techniques like these. Now approved by regulatory authorities, drugs like nirmatrelvir/ritonavir are quite accessible, as long as you have an HCP’s prescription. They’ve even surpassed supportive treatments and taken center stage as the first line of defense against an active COVID-19 infection due to their efficacy and reliability. Nonetheless, HCPs can use all of these treatment types in tandem to make their combined impact more effective.
Despite all of their advantages, antiviral drugs don’t replace other infection control tactics. Patients using COVID-19 medications are still advised to self-isolate until their infection resolves or, if that’s not an option, wear a mask and practice social distancing. Here, let’s also note that these medications only treat existing cases; they don’t do anything to protect patients against future COVID-19 infection. Instead, those prevention measures are best addressed using vaccines and prophylaxis, two tactics we’ll explore later in this mini-series, as well as old school strategies like good hand hygiene. The classics never go out of style!
結論
The worst of the COVID-19 pandemic has now passed, but epidemiology demonstrates the constant skirmish between the scientific tools underlying public health and the increasing fortitude of formidable pathogens. As we anticipate future pandemics, we can plan ahead by reflecting on our past successes and shortfalls, and now we have effective treatments in case new COVID-19 cases recur in the future. These treatments, though challenging to invent and deploy, represent a great achievement in the biomedical research realm. Although we can’t fully cure viral infections, the good news is that we can prevent them. In a forthcoming article in this public health mini-series, we’ll explore the advanced array of preventive measures — including the groundbreaking mRNA vaccine technology — that stopped COVID-19’s spread in its tracks.
What happens in the body between the time patients are prescribed COVID-19 medications and the time they start to feel better?